Note: this article pertains to kidney donation in the United States. Each country has its own idiosyncratic approach to dealing with nondirected donations, so your mileage from reading this article may vary.
TL;DR: becoming a living kidney donor is an amazing way to have a positive impact on another person at limited cost to yourself. Each year, 43,000 people die needlessly from kidney disease. By becoming a nondirected donor, you can give someone on the transplant waiting list their life back.
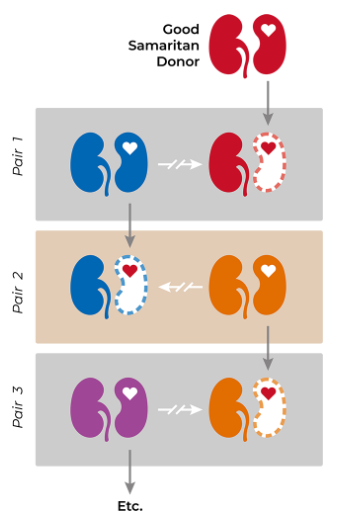
In fact, a nondirected kidney donation is often able to free up unmatched pairs in the National Kidney Registry (NKR) system. In this way, your donation may have an impact beyond the recipient and his or her community. By going first and expecting nothing in return, a nondirected kidney donor can enable a chain of donations that saves dozens (maybe many dozens!) of lives.
Through nondirected kidney donation, you can reduce the suffering of another person, ending their dependence on dialysis and hopefully providing them with many years of health. On average, a kidney from a living donor can be expected to function for 12 to 20 years, whereas a kidney from deceased donor tends to function for 8 to 12 years (source).
Donating a kidney is considered a major surgery. There is a risk of complications and no positive benefit for the donor. And yet, people who have donated a kidney outlive the average person. (Probably selection effects: potential donors need to have good overall health in order to be eligible.)
1 ) The Case against Nondirected Donation
Obviously, becoming a living kidney donor is not right for everyone. For example, if you have a family history of kidney disease, there are much better ways you can work towards doing good.
If you're of good health with no familial history of kidney problems, you might be interested to know that the process is much less invasive, uncomfortable, and risky than you might have anticipated. There are no restrictions on what you can and cannot do after recovery. I'll talk more about this in the section below.
The most significant cost to potential donors is time. Getting approval to actually donate is quite time consuming. And for good reason: the transplant hospital wants to ensure that your kidney function is sufficient that you can drop to half capacity and still be okay. (In time, the donor's remaining kidney will grow stronger and take on much of the functioning of the kidney that was removed).
I would estimate the full process of kidney donation takes about 52 hours.
| Activity | Hr | Notes |
| Initial Call | 1 | Connect with Transplant Coordinator / fill out initial paperwork |
| Initial Visits | 0.5 | At home labs (i.e., peeing in a jug) |
| Initial Visits | 4 | Radiology + MRI + PET scan + X-Rays + labs |
| Initial Visits - transportation | 1.5 | Getting to transplant center, finding parking, finding your first appointment, etc. |
| Follow Up Evaluation | 4 | Conversations with social worker, psych, nephrologist, other |
| Acceptance | 4 | Paperwork (i.e., Donor Shield, notifying job, getting STD through job) |
| Surgery Prep | 0.5 | Thoroughly washing surgical site in advance of surgery |
| Surgery - transportation | 1.5 | Getting to transplant center, finding parking, finding surgery center |
| Surgery | 29 | In hospital for 36 hours - 7 hours you would have been sleeping anyway |
| Follow Up Visits and Labs | 6 | Conducted over Zoom / at PCP's office during normal checkups |
| Total | 52 |
For some EAs, it may be more effective to use these 52 hours for something else - like more time working their EA job or earning to give.
For example, if you can find work that earns $65 / hour after taxes, your 52 hours of extra work translates to approximately one life saved through neartermist global health philanthropy. No need to undergo the discomfort of becoming a kidney donor.
However, it seems unlikely that the average person will use 52 marginal hours of free time in a way that's more effective than kidney donation.
2 ) The Case for Nondirected Donation
For what it's worth, there are also several benefits that accrue to the donor throughout this process, such as a comprehensive free kidney-function checkup, cash offsets from Donor Shield, time off work through FMLA, and short term disability payments. Laws and policies do a good job of defraying some of the costs associated with the choice to donate.
The Family Voucher Program, for example, removes one potential disincentive for donors related to worry about friends and families. This program allows you to select five friends / family members, and then if any one of these five individuals needs a kidney transplant later in life, they're moved to the top of the list. (Note that this is a "first come, first served" deal - once one voucher recipient receives a transplant, the rest of the vouchers are invalidated. Also note that this doesn't solve for the situation where the donor's future spouse, child, or close friend they haven't met yet needs a kidney - the vouchers must be allocated in advance of donation).
Similarly, the donor would also be moved to the top of the waiting list in the unlikely event he or she needed a kidney later in life. It seems that the risk of kidney failure for kidney donors goes up roughly 1 percentage point.
As explained at the top, living kidney donation isn't going to be a good fit for every person. However, I am convinced that 43,000 people should step up each year to end the needless suffering associated with kidney disease. If you're willing to be patient with hospital logistics, and you're willing to undergo a bit of physical discomfort, kidney donation is an amazing opportunity.
3 ) My Personal Experience as a Kidney Donor through NKR
In August of 2021, I donated my kidney to a stranger through the National Kidney Registry (NKR) at MedStar Georgetown in Washington, DC. This section outlines my experience for anyone who's still curious about what the process looks like.
I first heard about the opportunity to become a living kidney donor in winter of late 2016 or early 2017 through a radio spot on NPR, which also mentioned Peter Singer's The Life You Can Save. I immediately decided this was something I wanted to learn more about.
There isn't exactly a Yelp for picking the hospital where you donate, so my best advice is to reach out to the EA community to see if other people have had experience at the transplant center you're considering.
Getting accepted as a donor requires blood tests, x-ray of the chest, CT of the abdomen, psychiatric eval, and peeing in a jar for 48 hours to check your creatine levels. Not pleasant, but important to ensure you're of above average overall health and kidney function.
When all the tests clear, you can schedule the surgery. Ideally, NKR will set you up such that your donation sets off a chain. Ultimately, the scheduling is donor-centric, so it's completely up to you to determine when you feel ready to undergo the procedure and resulting six-week recovery. As you plan to take time off work, your coordinator should provide info about NKR's Donor Shield. I was also eligible for DC's FMLA and Short Term Disability from my workplace.
Before surgery, some friends threw me a Kidney Graduation Party at a local park. This was extremely sweet, and I think it's something all kidney donors should consider organizing as an opportunity to celebrate and normalize the act of donation.
On the day of surgery, I arrived at MedStar at 5am, and was unconscious by about 7:15am. My kidney was removed laparoscopically and sent to the recipient in Indiana. I passed the afternoon loopily browsing the book I'd brought to the hospital and texting friends and family to let them know I was okay. After an overnight snooze and some broth that left me surprisingly hungry, at 12pm I was released from the hospital. After 36 hours in the hospital, my energy and appetite were significant.
The next couple days, I continued to feel pretty much fine. I ran errands on foot and did some work towards personal goals. When it occurred, discomfort was fleeting. The worst I experienced was infrequent nerve pain in my shoulders from gas used during surgery. Also, anything that involved a 'crunch' motion of the abs sent lightning across the incision sites. (So rather than bending over to pick up a dropped object, I opted to do a kind of sumo squat so that I could keep my back straight.) Getting in and out of bed was a momentary inconvenience. But these moments of discomfort resolved themselves within a few days. I never experienced nausea or any sensation in my abdomen as my organs resettled.
And that's basically it in terms of recovery! The only other challenge was not to workout or carry anything heavier than 10 pounds during the six weeks after surgery. Listen to your doctor and to your body as you return to your previous level of activity after six weeks.
As an avid runner, I started with elliptical, then some three mile jogs, and gradually built up my weekly mileage. Two and a half months out from surgery, I ran a virtual half marathon in support of Kidney Transplant Thursday. My mile splits averaged 8:20 - not a PR, but on par with halfs I'd run in college.
Nearly a year out from donation, I've had no issues associated with the decision to part with one of my kidneys. I strongly recommend nondirected donation if you're a healthy person with the time to dedicate to the process.
Great post, and I'm a little sad that kidney donation has fallen a bit out of EA discussions. I also want to emphasize two things to people who are worried about the health risks from donating their kidney.
As the OP says, you have to have substantially above average kidney functioning in order to be eligible. I recall seeing estimates that because of this screening, living donors are actually at lower risk for kidney disease than the general US population. But I can't find them so take that with a grain of salt.
Being a living kidney donor sends you to the top of transplant lists, so in the extremely unlikely event that you do have kidney problems, you are far more likely than average to receive a transplant quickly.
When I looked into this, I came away with the impression that this is not true. According to the formal requirements, you don't need to have above average kidney function to be eligible. You need to not have a recorded history of kidney disease and take a test that weakly indicates that you are currently in the healthy range.
The healthy range isn't tied to your age. A young person with healthy kidney function can expect to probably have reduced kidney function in old age. The cut off for donation is a GFR of 90 (though doctors can accept patients as low as 60 in some cases). If your GFR is 90 and you're 80 years old, you've got great kidney function. If your GFR is 90 and you're 30, you don't have to worry about kidney problems now, but you may have reason to be wary about the future.
For the purposes of donation, your kidney function is measured by creatinine clearance. This is an easy test to do, but isn't particularly accurate. Your measurement can change significantly from test to test. There may be significant racial and dietary effects that aren't considered in the process.
Current kidney function isn't a fantastic guide to future kidney function. Your kidneys can work at different levels. Their full capacity is a function of their nephron count and it is hugely variable between individuals. If you don't have a lot of nephrons but they're working overtime, you might have a high GFR even though your prospects for the future aren't great. There is no good way to assess your nephron count.
Individual doctors have leeway to reject people who they think are at particular risk, but they have moral and financial incentives to err on the side of accepting borderline acceptable candidates and the formal requirements don't require exceptional kidney function.
Some nuance here... First, every transplant center has different protocol in how they determine eligibility. There are some general basic requirements nearly all centers follow but beyond that there's a lot of variability.
Second, NKR leads the world in donor protections. NKR-affiliated transplant centers have better outcomes all around. They tend to do better, more thorough donor screenings. You can evaluate transplant centers here: https://www.kidneytransplantcenters.org/
About GFR, most equations (whether they are creatinine based or cystatin-c) do in fact use age to adjust. And many centers will run both tests, as well as additional tests like a nuclear renal scan to determine kidney function, size, etc. There are no clear ways to determine the future but there are lots of tests that indicate whether someone is a high or low risk for future kidney disease.
Also regarding age, there is a good reason most centers prefer to take kidneys out of middle age people rather than young people: life habits are more strongly established and future health is easier to estimate because many of the most risky activities the person will engage in are in the past.
Regarding the need/idea of "exceptional kidney function." Most humans living in societies with modern medicine do not need two kidneys; most can live just fine with partial function of one kidney.
You are right to worry about future kidney health, particularly in the age of poor public health and pandemics. For instance, I believe there is a high likelihood that CKD will increase among donors who have caught COVID. And hospital-acquired COVID is not even reliably discussed in the data yet, so making a decision NOW about becoming a living kidney donor is definitely more of a gamble than it was pre-pandemic.
Every transplant center has an evaluation team. It is never just an individual doctor who makes a decision about a candidate. This is good and bad in my opinion, but it speaks to your last point about incentives.
Personally my experience felt like there were a lot of roadblocks to becoming a donor; they don't make it easy. Someone needs to be pretty motivated to even get to the point where the team makes a decision and by then you have had access to all of your test results so you can consult with other doctors if you wish.
For the record, the screening process is not just looking at kidney health. It's also looking for cancers, heart health, etc. They are looking for anything that could make your surgery dangerous, anything that could harm your recipient, and anything that suggests longterm negative health consequences for you post-surgery. They have strong incentives to keep their rankings high with good outcomes and I believe those incentives outweigh any incentives you mentioned.
Hi Nicole,
I think this is a cool choice and a good post - thanks for both! I agree with your bottom line that kidney donation can be a good choice for EAs and just wanted to flag a few additional resources and considerations:
Thank you for your comment, Alexander!
I don't have a particularly good estimate on total time, but my impression is that most doctors recommend people plan to take a couple weeks off from office work, which would maybe 2-3x your 52 hr estimate?
Thanks for writing this Nicole!
Agree about 2ish weeks off work as the standard, though Alexander and I donated ~ten years ago, and I have some (purely anecdotal) sense that the surgery experience (and recovery) for people like Nicole who've donated since then at a big center might be better.
Also, I think this Annals of Internal Medicine meta-analysis on the risks of kidney donation is a good resource for people who feel comfortable reading academic papers.
Since I was able to be productive right away on personal projects and errands, I didn't count this time in my estimate.
I used my time off to learn JavaScript well enough to eventually switch careers from Data Scientist to Frontend Developer, so it was a pretty fruitful period for me.
I would estimate the time I spent for my living kidney donation to be much bigger than 52 hours as well. A lot of that is because I spent significant time ensuring that I was as protected as possible. Also because my donation was interrupted by COVID.
First I would count my time in research to determine which hospital I wanted to go through as well as all my travel time to visit that hospital because it was out of state (my state has zero NKR affiliated hospitals and only did 6 living donor transplants last year - am I going to trust them to do mine? NO!)
Next, I went through the process, was approved, then COVID hit. Enough time went by that I had to do the entire evaluation process over again. Each evaluation process easily took AT LEAST 52 hours for me because each time involved a two-day testing process plus travel plus additional local tests.
Then time was wasted when my coordinator got COVID and couldn't put my case up for approval. Last minute extra tests - partially BECAUSE OF COVID - added to the time I spent doing this.
Lastly, I spent extra time nearby the hospital after surgery in order to obey their recommendations that I stay local in case complications arise but also I did this to kickstart my recovery by eliminating my normal life responsibilities. It worked beautifully and I am recovering very well. But I know that if I hadn't taken that time off it likely would have impeded my recovery.