Stan Pinsent
Bio
Participation3
Director of Research at CEARCH: https://exploratory-altruism.org/
I construct cost-effectiveness analyses of various cause areas, identifying the most promising opportunities for impactful work.
Previously a teacher in London, UK.
Posts 21
Comments100
Topic contributions1
Thanks for the detailed response, Vasco! Apologies in advance that this reply is slightly rushed and scattershot.
I agree that you are right with the maths - it is 251x, not 63,000x.
- I am not comparing the cost-effectiveness of preventing events of different magnitudes.
- Instead, I am comparing the cost-effectiveness of saving lives in periods of different population losses.
OK, I did not really get this!
In your example on wars you say
- As a consequence, if the goal is minimising war deaths[2], spending to save lives in wars 1 k times as deadly should be 0.00158 % (= (10^3)^(-1.6)) as large.
Can you give an example of what might count as "spending to save lives in wars 1k times as deadly" in this context?
I am guessing it is spending money now on things that would save lives in very deadly wars. Something like building a nuclear bunker vs making a bullet proof vest? Thinking about the amounts we might be willing to spend on interventions that save lives in 100-death wars vs 100k-death wars, it intuitively feels like 251x is a way better multiplier than 63,000. So where am I going wrong?
When you are thinking about the PDF of , are you forgetting that ∇ is not proportional to ∇?
To give a toy example: suppose .
Then if we have
If we have
The "height of the PDF graph" will not capture these differences in width. This won't matter much for questions of 100 vs 100k deaths, but it might be relevant for near-existential mortality levels.
Using PDF rather than CDF to compare the cost-effectiveness of preventing events of different magnitudes here seems off.
You show that preventing (say) all potential wars next year with a death toll of 100 is 1000^1.6 = 63,000 times better in expectation than preventing all potential wars with a death toll of 100k.
More realistically, intervention A might decrease the probability of wars of magnitude 10-100 deaths and intervention B might decrease the probability of wars of magnitude 100,000 to 1,000,000 deaths. Suppose they decrease the probability of such wars over the next n years by the same amount. Which intervention is more valuable? We would use the same methodology as you did except we would use the CDF instead of the PDF. Intervention A would be only 1000^0.6 = 63 times as valuable.
As an intuition pump we might look at the distribution of military deaths in the 20th century. Should the League of Nations/UN have spent more effort preventing small wars and less effort preventing large ones?
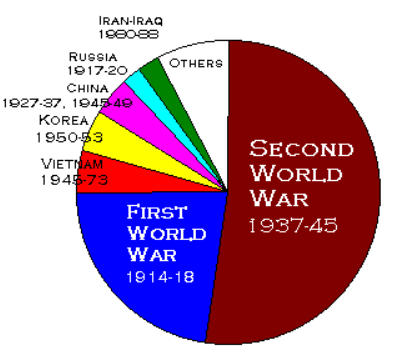
The data actually makes me think that even the 63x from above is too high. I would say that in the 20th century, great-power conflict > interstate conflict > intrastate conflict should have been the order of priorities (if we wish to reduce military deaths). When it comes to things that could be even deadlier than WWII, like nuclear war or a pandemic, it's obvious to me that the uncertainty about the death toll of such events increases at least linearly with the expected toll, and hence the "100-1000 vs 100k-1M" framing is superior to the PDF approach.
I welcome this idea! More love would be a good thing, and we would rather make this change earlier in the life course.
I think implementation is hard. This is a big "if":
if we could come up with a healthy, inclusive (but respectful of differing opinions), curriculum that -encourages/rewards- love but does not impose it
As Joseph said, it is difficult to assess educational interventions. When it comes to knowledge transfer we can be generally confident that education is helping - calculus classes increase students' aptitude for calculus. But love?
Recent research suggests that mindfulness interventions in schools were much less impactful than hoped. I suspect that something like mindfulness works well if you opt in - and is much less useful if you didn't ask for it.
To explore this idea further, I recommend looking for comparable values-based educational experiments that have been tried in the past (maybe something about attitudes to sexuality, or religious tolerance, or positive thinking, or even campaigns to instil hate). Did they succeed in changing values? If they failed, why did they fail? If they succeeded, what can we learn from them?
my guess is [...] you could counterfactually save 1-5 more lives per day by volunteering and being great at your job.
I'm skeptical. That would mean that your average hotline volunteer is speaking to 1-5 new people per day who subsequently take their lives, but would not have if the call were handled better. This seems implausible purely on the basis that most suicide attempts fail (5-11% of people who ever attempt end up ever succeeding). Added to this, I suspect that some (most?) people who call are thinking about suicide but not literally about to do it, some (most?) are making multiple calls to the hotline, and that some of the worst cases may be possible to save today but will take their lives in a few months' time. Basically, I suspect that each call that a volunteer successfully handles would be worth more like 0.001 or 0.01 of an averted suicide.
I did (non-suicide) helpline training once and was struck by how formalised it is. Volunteers were supposed to be listeners, reflecting the callers' thoughts back to them and avoiding giving advice. This is likely a strategy to minimise the harm caused by layperson volunteers interacting with very vulnerable people. I would suspect that suicide hotlines have fairly rigid guidelines on how to handle calls, probably with more specific training on how to help the caller de-escalate their suicidal thoughts in the moment. My concern would be that this leaves little wiggle room for being "great at your job", and anyone trying to be significantly more effective may actually do damage by going off-script.
Would love to hear from someone with direct experience!
Great summary!
There is also a mental health benefit to averting unwanted pregnancy. A meta-analysis by Wang et al. (2021) found that women with an unplanned pregnancy were 62% more likely (28% vs. 17%) to suffer postpartum depression compared to women with a planned pregnancy. We don't have good data on depression prevalence among women whose unplanned pregnancy was averted, but it seems probable that an unplanned pregnancy increases the risk of mental illness, even if only by adding another life stressor. It is very hard to measure, but I suspect that the wellbeing benefits of not having one's education cut short / career & income disrupted / living with stigma of being a single mother or with a partner you didn't choose to have a child with / etc. are high.
I think this is a good way of trying to secure strong counterfactual impact. I notice that your cost-effectiveness estimates imply that you prevent 200 maternal deaths per 100,000 averted pregnancies. How do you arrive at this figure, given the lack of maternal mortality data for your specific demographic (unwanted pregnancy, rural, underserved, low-income country)? Nigeria has the 2nd-worst maternal mortality rate in the world, at 112 per 100,000 - but your Nigeria numbers suggest something like 500 per 100,000.
Another interesting thing is that you avert a maternal death for $3,353 - which means maybe $70-100 per extra year of life that these women get - and you avert a DALY for $4.77. This implies that averted maternal deaths only account for ~5% of the health benefits you are measuring. Where are the other 95% coming from? Importantly, are any coming from the infant or from non-health benefits converted into DALYs - because counting these would be moral assumptions worth flagging.